Recently, extensive studies have shown that ferroptosis boosted a perspective for its usage in cancer therapeutics. The current study aims to construct a robust ferroptosis-related lncRNAs signature prediction model to increase the predicted value of colorectal cancer (CRC) by bioinformatics analysis. By comparing CRC tissue with adjacent normal tissues, we screened 2541 differentially expressed lncRNAs from The Cancer Genome Atlas (TCGA) CRC using the R language and "limma" package, of which 439 are ferroptosis-related lncRNAs. Univariate Cox regression, lasso regression, multivariate Cox regression are used to construct a seven ferroptosis-related lncRNAs (AC005550.2, LINC02381, AL137782.1, C2orf27A, AC156455.1, AL354993.2, AC008760.1) prognostic signature in train set. This model's prognosis in the high-risk group is worse than that of the low-risk group in the train set, test set, and entire set. Based on the stratification of clinical variables (gender, age, clinical stage, postoperative tumor status, CEA levels, perineural invasion, vascular invasion, mismatch repair (MMR) and gene mutation status (KRAS, BRAF)), the high-risk group's prognosis is also worse than that of the low-risk group. The area under curve (AUC) of receiver operating characteristic (ROC) curve for predicting three years survival in the train set, test set, and entire set were 0.796, 0.715, and 0.758, respectively. Furthermore, Univariate Cox regression and multivariate Cox regression displayed that the signature could serve as an independent prognostic factor; meanwhile, we draw the nomogram based on multivariate Cox regression (P<0.05). Compared to clinical variables, this signature's ROC curves demonstrated the second largest AUC value (0.737). The expression of these lncRNAs and the lncRNA signature are related to clinical stage, T stage, Lymph-node status, distant metastasis, KRAS mutation, BRAF mutation, MMR status, and perineural invasion. Finally, GSEA analysis results show that the signature is involved in six KEGG signal pathways, such as KEGG_HEDGEHOG_SIGNALING_PATHWAY, KEGG_ALPHA_LINOLENIC_ACID_METABOLISM, KEGG_ARACHIDONIC_ACID_METABOLISM, KEGG_CITRATE_CYCLE_TCA_CYCLE, KEGG_PENTOSE_PHOSPHATE_PATHWAY, KEGG_FRUCTOSE_AND_MANNOSE_METABOLISM. In conclusion, the current study shows a seven ferroptosis-related lncRNA signature could efficiently function as a novel and independent prognosis biomarker and therapeutic target for CRC patients.
| Published in | Cancer Research Journal (Volume 13, Issue 1) |
| DOI | 10.11648/j.crj.20251301.12 |
| Page(s) | 9-22 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
lncRNA, TCGA, Ferroptosis, Colorectal Cancer, Signature
Clinical variables | Case | Percentage |
|---|---|---|
Gender | ||
Male | 242 | 46.36% |
Female | 280 | 53.64% |
Age (years) | ||
Range | 33-88 | |
Median | 66 | |
Race | ||
ASIAN | 8 | 1.53% |
BLACK | 53 | 10.15% |
AMERICAN INDIAN | 1 | 0.19% |
WHITE | 393 | 75.29% |
unknow | 67 | 12.84% |
Clinical Stage | ||
Stage I | 279 | 53.45% |
Stage II | 124 | 23.75% |
Stage III | 85 | 16.28% |
Stage IV | 26 | 4.98% |
unknow | 8 | 1.53% |
T stage | ||
T1+Tis | 172 | 32.95% |
T2 | 281 | 53.83% |
T3 | 47 | 9.00% |
T4 | 19 | 3.64% |
Tx | 3 | 0.57% |
Lymph node status | ||
N0 | 335 | 64.18% |
N1 | 98 | 18.77% |
N2 | 75 | 14.37% |
N3 | 2 | 0.38% |
Nx+unknow | 12 | 2.30% |
Metastasis | ||
M0 | 353 | 67.62% |
M1 | 25 | 4.79% |
Mx+unknow | 144 | 27.59% |
Eml4-Alk translocation status | ||
Yes | 34 | 6.51% |
No | 213 | 40.80% |
unknow | 275 | 52.68% |
EGFR mutation status | ||
Yes | 80 | 15.33% |
NO | 197 | 37.74% |
unknow | 285 | 54.60% |
KRAS mutation status | ||
Yes | 62 | 11.88% |
No | 253 | 48.47% |
unknow | 207 | 39.66% |
Postoperative tumor status | ||
WITH TUMOR | 111 | 21.26% |
TUMOR FREE | 314 | 60.15% |
unknow | 97 | 18.58% |
History neoadjuvant treatment | ||
Yes | 3 | 0.57% |
No | 518 | 99.23% |
unknow | 1 | 0.19% |
Clinical features | univariate Cox regression | multivariate Cox regression | ||||||
|---|---|---|---|---|---|---|---|---|
HR | HR.95L | HR.95H | pvalue | HR | HR.95L | HR.95H | pvalue | |
Age (continuous variable) | 0.997 | 0.978 | 1.015 | 0.718 | 1.003 | 0.984 | 1.023 | 0.738 |
Gender | 1.000 | 0.694 | 1.441 | 1.000 | 1.213 | 0.828 | 1.775 | 0.322 |
Clinical stage | 1.648 | 1.396 | 1.946 | 0.000 | 1.985 | 1.241 | 3.175 | 0.004 |
T stage | 1.600 | 1.285 | 1.994 | 0.000 | 1.155 | 0.909 | 1.468 | 0.237 |
Distant metastasis | 1.748 | 0.959 | 3.187 | 0.068 | 0.395 | 0.118 | 1.319 | 0.131 |
Lymph-node status | 1.787 | 1.455 | 2.195 | 0.000 | 0.992 | 0.665 | 1.481 | 0.970 |
An eight ferroptosis-related lncRNAs signature | 1.039 | 1.022 | 1.058 | 0.000 | 1.040 | 1.020 | 1.061 | 0.000 |
CRC | Colorectal Cancer |
GSEA | Gene Set Enrichment Analysis |
FDR | False Discovery Rate |
OS | Overall Survival |
HRs | Hazard Ratios |
CI | Confidence Interval |
TCGA | The Cancer Genome Atlas |
AUC | Area Under Curve |
ROC | Receiver Operating Characteristic |
KEGG | Kyoto Encyclopedia of Genes and Genomes |
| [1] | Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021; 71(3): 209-249. |
| [2] | Ferlay J, Steliarova-Foucher E, Lortet-Tieulent J, et al. Cancer incidence and mortality patterns in Europe: estimates for 40 countries in 2012. Eur J Cancer. 2013; 49(6): 1374-1403. |
| [3] | Dixon SJ, Lemberg KM, Lamprecht MR, et al. Ferroptosis: an iron-dependent form of nonapoptotic cell death. Cell. 2012; 149(5): 1060-1072. |
| [4] | Yang WS, SriRamaratnam R, Welsch ME, et al. Regulation of ferroptotic cancer cell death by GPX4. Cell. 2014; 156(1-2): 317-331. |
| [5] | Li J, Cao F, Yin HL, et al. Ferroptosis: past, present and future. Cell Death Dis. 2020; 11(2): 88. Published 2020 Feb 3. |
| [6] | Fearnhead HO, Vandenabeele P, Vanden Berghe T. How do we fit ferroptosis in the family of regulated cell death?. Cell Death Differ. 2017; 24(12): 1991-1998. |
| [7] | Sui X, Zhang R, Liu S, et al. RSL3 Drives Ferroptosis Through GPX4 Inactivation and ROS Production in Colorectal Cancer. Front Pharmacol. 2018; 9: 1371. Published 2018 Nov 22. |
| [8] | Chen P, Li X, Zhang R, et al. Combinative treatment of β-elemene and cetuximab is sensitive to KRAS mutant colorectal cancer cells by inducing ferroptosis and inhibiting epithelial-mesenchymal transformation. Theranostics. 2020; 10(11): 5107-5119. Published 2020 Apr 6. |
| [9] |
Shen LD, Qi WH, Bai JJ, et al. Resibufogenin inhibited colorectal cancer cell growth and tumorigenesis through triggering ferroptosis and ROS production mediated by GPX4 inactivation [retracted in: Anat Rec (Hoboken). 2021 Dec; 304(12): 2892.
https://doi.org/10.1002/ar.24378 ]. Anat Rec (Hoboken). 2021; 304(2): 313-322. |
| [10] | Sharma P, Shimura T, Banwait JK, Goel A. Andrographis-mediated chemosensitization through activation of ferroptosis and suppression of β-catenin/Wnt-signaling pathways in colorectal cancer. Carcinogenesis. 2020; 41(10): 1385-1394. |
| [11] | Park S, Oh J, Kim M, Jin EJ. Bromelain effectively suppresses Kras-mutant colorectal cancer by stimulating ferroptosis. Anim Cells Syst (Seoul). 2018; 22(5): 334-340. Published 2018 Aug 30. |
| [12] | Zhang L, Liu W, Liu F, et al. Corrigendum to "IMCA Induces Ferroptosis Mediated by SLC7A11 through the AMPK/mTOR Pathway in Colorectal Cancer". Oxid Med Cell Longev. 2020; 2020: 6901472. Published 2020 Oct 27. |
| [13] | Xia Y, Liu S, Li C, et al. Discovery of a novel ferroptosis inducer-talaroconvolutin A-killing colorectal cancer cells in vitro and in vivo. Cell Death Dis. 2020; 11(11): 988. Published 2020 Nov 17. |
| [14] | Lu D, Yang Z, Xia Q, et al. ACADSB regulates ferroptosis and affects the migration, invasion, and proliferation of colorectal cancer cells. Cell Biol Int. 2020; 44(11): 2334-2343. |
| [15] | Xu X, Zhang X, Wei C, et al. Targeting SLC7A11 specifically suppresses the progression of colorectal cancer stem cells via inducing ferroptosis. Eur J Pharm Sci. 2020; 152: 105450. |
| [16] | Sun J, Cheng X, Pan S, et al. Dichloroacetate attenuates the stemness of colorectal cancer cells via trigerring ferroptosis through sequestering iron in lysosomes. Environ Toxicol. 2021; 36(4): 520-529. |
| [17] | Malfa GA, Tomasello B, Acquaviva R, et al. Betula etnensis Raf. (Betulaceae) Extract Induced HO-1 Expression and Ferroptosis Cell Death in Human Colon Cancer Cells. Int J Mol Sci. 2019; 20(11): 2723. Published 2019 Jun 3. |
| [18] | Xian ZY, Hu B, Wang T, et al. CircABCB10 silencing inhibits the cell ferroptosis and apoptosis by regulating the miR-326/CCL5 axis in rectal cancer. Neoplasma. 2020; 67(5): 1063-1073. |
| [19] | Mercer TR, Dinger ME, Mattick JS. Long non-coding RNAs: insights into functions. Nat Rev Genet. 2009; 10(3): 155-159. |
| [20] | Quinn JJ, Chang HY. Unique features of long non-coding RNA biogenesis and function. Nat Rev Genet. 2016; 17(1): 47-62. |
| [21] | Mao C, Wang X, Liu Y, et al. A G3BP1-Interacting lncRNA Promotes Ferroptosis and Apoptosis in Cancer via Nuclear Sequestration of p53. Cancer Res. 2018; 78(13): 3484-3496. |
| [22] | Qi W, Li Z, Xia L, et al. LncRNA GABPB1-AS1 and GABPB1 regulate oxidative stress during erastin-induced ferroptosis in HepG2 hepatocellular carcinoma cells. Sci Rep. 2019; 9(1): 16185. Published 2019 Nov 7. |
| [23] | Wang M, Mao C, Ouyang L, et al. Correction to: Long noncoding RNA LINC00336 inhibits ferroptosis in lung cancer by functioning as a competing endogenous RNA. Cell Death Differ. 2020; 27(4): 1447. |
| [24] | Wang Z, Chen X, Liu N, et al. A Nuclear Long Non-Coding RNA LINC00618 Accelerates Ferroptosis in a Manner Dependent upon Apoptosis. Mol Ther. 2021; 29(1): 263-274. |
| [25] | Gai C, Liu C, Wu X, et al. MT1DP loaded by folate-modified liposomes sensitizes erastin-induced ferroptosis via regulating miR-365a-3p/NRF2 axis in non-small cell lung cancer cells. Cell Death Dis. 2020; 11(9): 751. Published 2020 Sep 14. |
| [26] | Ritchie ME, Phipson B, Wu D, et al. limma powers differential expression analyses for RNA-sequencing and microarray studies. Nucleic Acids Res. 2015; 43(7): e47. |
| [27] | Simon N, Friedman J, Hastie T, Tibshirani R. Regularization Paths for Cox's Proportional Hazards Model via Coordinate Descent. J Stat Softw. 2011; 39(5): 1-13. |
| [28] | Groeneveld CS, Chagas VS, Jones SJM, et al. RTNsurvival: an R/Bioconductor package for regulatory network survival analysis. Bioinformatics. 2019; 35(21): 4488-4489. |
| [29] | Heagerty PJ, Lumley T, Pepe MS. Time-dependent ROC curves for censored survival data and a diagnostic marker. Biometrics. 2000; 56(2): 337-344. |
| [30] | Subramanian A, Tamayo P, Mootha VK, et al. Gene set enrichment analysis: a knowledge-based approach for interpreting genome-wide expression profiles. Proc Natl Acad Sci U S A. 2005; 102(43): 15545-15550. |
| [31] | Adam R, de Gramont A, Figueras J, et al. Managing synchronous liver metastases from colorectal cancer: a multidisciplinary international consensus. Cancer Treat Rev. 2015; 41(9): 729-741. |
| [32] | Bhan A, Soleimani M, Mandal SS. Long Noncoding RNA and Cancer: A New Paradigm. Cancer Res. 2017; 77(15): 3965-3981. |
| [33] | Liang JY, Wang DS, Lin HC, et al. A Novel Ferroptosis-related Gene Signature for Overall Survival Prediction in Patients with Hepatocellular Carcinoma. Int J Biol Sci. 2020; 16(13): 2430-2441. Published 2020 Jul 6. |
| [34] | Zhuo S, Chen Z, Yang Y, Zhang J, Tang J, Yang K. Clinical and Biological Significances of a Ferroptosis-Related Gene Signature in Glioma. Front Oncol. 2020; 10: 590861. Published 2020 Nov 20. |
| [35] | Yang G, Zhang Y, Yang J. A Five-microRNA Signature as Prognostic Biomarker in Colorectal Cancer by Bioinformatics Analysis. Front Oncol. 2019; 9: 1207. Published 2019 Nov 12. |
| [36] | Bai J, Zhang X, Xiang ZX, Zhong PY, Xiong B. Identification of prognostic immune-related signature predicting the overall survival for colorectal cancer. Eur Rev Med Pharmacol Sci. 2020; 24(3): 1134-1141. |
| [37] | Zhang J, Cheng X, Wang J, Huang Y, Yuan J, Guo D. Gene signature and prognostic merit of M6a regulators in colorectal cancer. Exp Biol Med (Maywood). 2020; 245(15): 1344-1354. |
| [38] | Hu X, Li YQ, Ma XJ, Zhang L, Cai SJ, Peng JJ. A Risk Signature With Inflammatory and T Immune Cells Infiltration in Colorectal Cancer Predicting Distant Metastases and Efficiency of Chemotherapy. Front Oncol. 2019; 9: 704. Published 2019 Aug 13. |
| [39] | Tokunaga R, Nakagawa S, Sakamoto Y, et al. 12-Chemokine signature, a predictor of tumor recurrence in colorectal cancer. Int J Cancer. 2020; 147(2): 532-541. |
| [40] | Zong Z, Li H, Yi C, Ying H, Zhu Z, Wang H. Genome-Wide Profiling of Prognostic Alternative Splicing Signature in Colorectal Cancer. Front Oncol. 2018; 8: 537. Published 2018 Nov 20. |
| [41] | Li K, Zeng L, Wei H, et al. Identification of gene-specific DNA methylation signature for Colorectal Cancer. Cancer Genet. 2018; 228-229: 5-11. |
| [42] | Zhou Z, Mo S, Dai W, et al. Development and Validation of an Autophagy Score Signature for the Prediction of Post-operative Survival in Colorectal Cancer. Front Oncol. 2019; 9: 878. Published 2019 Sep 9. |
| [43] | Wu B, Tao L, Yang D, Li W, Xu H, He Q. Development of an Immune Infiltration-Related Eight-Gene Prognostic Signature in Colorectal Cancer Microenvironment. Biomed Res Int. 2020; 2020: 2719739. Published 2020 Aug 27. |
| [44] | Li Z, Wang D, Yin H. A seven immune-related lncRNA signature predicts the survival of patients with colon adenocarcinoma. Am J Transl Res. 2020; 12(11): 7060-7078. Published 2020 Nov 15. |
| [45] | Zhou W, Zhang S, Li HB, et al. Development of Prognostic Indicator Based on Autophagy-Related lncRNA Analysis in Colon Adenocarcinoma. Biomed Res Int. 2020; 2020: 9807918. Published 2020 Sep 2. |
| [46] | Jafarzadeh M, Soltani BM, Soleimani M, Hosseinkhani S. Epigenetically silenced LINC02381 functions as a tumor suppressor by regulating PI3K-Akt signaling pathway. Biochimie. 2020; 171-172: 63-71. |
| [47] | Jafarzadeh M, Soltani BM. Long Noncoding RNA LOC400043 (LINC02381) Inhibits Gastric Cancer Progression Through Regulating Wnt Signaling Pathway [retracted in: Front Oncol. 2023 Dec 05; 13: 1298859.]. Front Oncol. 2020; 10: 562253. Published 2020 Oct 23. |
| [48] | Chen X, Zhang Z, Ma Y, Su H, Xie P, Ran J. LINC02381 Promoted Cell Viability and Migration via Targeting miR-133b in Cervical Cancer Cells. Cancer Manag Res. 2020; 12: 3971-3979. Published 2020 May 26. |
| [49] | Wei J, Ge X, Tang Y, et al. An Autophagy-Related Long Noncoding RNA Signature Contributes to Poor Prognosis in Colorectal Cancer. J Oncol. 2020; 2020: 4728947. Published 2020 Oct 21. |
| [50] | Friedmann Angeli JP, Krysko DV, Conrad M. Ferroptosis at the crossroads of cancer-acquired drug resistance and immune evasion. Nat Rev Cancer. 2019; 19(7): 405-414. |
| [51] | Elgendy SM, Alyammahi SK, Alhamad DW, Abdin SM, Omar HA. Ferroptosis: An emerging approach for targeting cancer stem cells and drug resistance. Crit Rev Oncol Hematol. 2020; 155: 103095. |
APA Style
Zhang, Y., Yang, G., Wang, J., Duan, H. (2025). A Novel Ferroptosis-Related lncRNA Prognostic Signature for Colorectal Cancer by Bioinformatics Analysis. Cancer Research Journal, 13(1), 9-22. https://doi.org/10.11648/j.crj.20251301.12
ACS Style
Zhang, Y.; Yang, G.; Wang, J.; Duan, H. A Novel Ferroptosis-Related lncRNA Prognostic Signature for Colorectal Cancer by Bioinformatics Analysis. Cancer Res. J. 2025, 13(1), 9-22. doi: 10.11648/j.crj.20251301.12
AMA Style
Zhang Y, Yang G, Wang J, Duan H. A Novel Ferroptosis-Related lncRNA Prognostic Signature for Colorectal Cancer by Bioinformatics Analysis. Cancer Res J. 2025;13(1):9-22. doi: 10.11648/j.crj.20251301.12
@article{10.11648/j.crj.20251301.12,
author = {Yujiao Zhang and Guodong Yang and Jiping Wang and Huaxin Duan},
title = {A Novel Ferroptosis-Related lncRNA Prognostic Signature for Colorectal Cancer by Bioinformatics Analysis
},
journal = {Cancer Research Journal},
volume = {13},
number = {1},
pages = {9-22},
doi = {10.11648/j.crj.20251301.12},
url = {https://doi.org/10.11648/j.crj.20251301.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.crj.20251301.12},
abstract = {Recently, extensive studies have shown that ferroptosis boosted a perspective for its usage in cancer therapeutics. The current study aims to construct a robust ferroptosis-related lncRNAs signature prediction model to increase the predicted value of colorectal cancer (CRC) by bioinformatics analysis. By comparing CRC tissue with adjacent normal tissues, we screened 2541 differentially expressed lncRNAs from The Cancer Genome Atlas (TCGA) CRC using the R language and "limma" package, of which 439 are ferroptosis-related lncRNAs. Univariate Cox regression, lasso regression, multivariate Cox regression are used to construct a seven ferroptosis-related lncRNAs (AC005550.2, LINC02381, AL137782.1, C2orf27A, AC156455.1, AL354993.2, AC008760.1) prognostic signature in train set. This model's prognosis in the high-risk group is worse than that of the low-risk group in the train set, test set, and entire set. Based on the stratification of clinical variables (gender, age, clinical stage, postoperative tumor status, CEA levels, perineural invasion, vascular invasion, mismatch repair (MMR) and gene mutation status (KRAS, BRAF)), the high-risk group's prognosis is also worse than that of the low-risk group. The area under curve (AUC) of receiver operating characteristic (ROC) curve for predicting three years survival in the train set, test set, and entire set were 0.796, 0.715, and 0.758, respectively. Furthermore, Univariate Cox regression and multivariate Cox regression displayed that the signature could serve as an independent prognostic factor; meanwhile, we draw the nomogram based on multivariate Cox regression (P<0.05). Compared to clinical variables, this signature's ROC curves demonstrated the second largest AUC value (0.737). The expression of these lncRNAs and the lncRNA signature are related to clinical stage, T stage, Lymph-node status, distant metastasis, KRAS mutation, BRAF mutation, MMR status, and perineural invasion. Finally, GSEA analysis results show that the signature is involved in six KEGG signal pathways, such as KEGG_HEDGEHOG_SIGNALING_PATHWAY, KEGG_ALPHA_LINOLENIC_ACID_METABOLISM, KEGG_ARACHIDONIC_ACID_METABOLISM, KEGG_CITRATE_CYCLE_TCA_CYCLE, KEGG_PENTOSE_PHOSPHATE_PATHWAY, KEGG_FRUCTOSE_AND_MANNOSE_METABOLISM. In conclusion, the current study shows a seven ferroptosis-related lncRNA signature could efficiently function as a novel and independent prognosis biomarker and therapeutic target for CRC patients.
},
year = {2025}
}
TY - JOUR T1 - A Novel Ferroptosis-Related lncRNA Prognostic Signature for Colorectal Cancer by Bioinformatics Analysis AU - Yujiao Zhang AU - Guodong Yang AU - Jiping Wang AU - Huaxin Duan Y1 - 2025/05/19 PY - 2025 N1 - https://doi.org/10.11648/j.crj.20251301.12 DO - 10.11648/j.crj.20251301.12 T2 - Cancer Research Journal JF - Cancer Research Journal JO - Cancer Research Journal SP - 9 EP - 22 PB - Science Publishing Group SN - 2330-8214 UR - https://doi.org/10.11648/j.crj.20251301.12 AB - Recently, extensive studies have shown that ferroptosis boosted a perspective for its usage in cancer therapeutics. The current study aims to construct a robust ferroptosis-related lncRNAs signature prediction model to increase the predicted value of colorectal cancer (CRC) by bioinformatics analysis. By comparing CRC tissue with adjacent normal tissues, we screened 2541 differentially expressed lncRNAs from The Cancer Genome Atlas (TCGA) CRC using the R language and "limma" package, of which 439 are ferroptosis-related lncRNAs. Univariate Cox regression, lasso regression, multivariate Cox regression are used to construct a seven ferroptosis-related lncRNAs (AC005550.2, LINC02381, AL137782.1, C2orf27A, AC156455.1, AL354993.2, AC008760.1) prognostic signature in train set. This model's prognosis in the high-risk group is worse than that of the low-risk group in the train set, test set, and entire set. Based on the stratification of clinical variables (gender, age, clinical stage, postoperative tumor status, CEA levels, perineural invasion, vascular invasion, mismatch repair (MMR) and gene mutation status (KRAS, BRAF)), the high-risk group's prognosis is also worse than that of the low-risk group. The area under curve (AUC) of receiver operating characteristic (ROC) curve for predicting three years survival in the train set, test set, and entire set were 0.796, 0.715, and 0.758, respectively. Furthermore, Univariate Cox regression and multivariate Cox regression displayed that the signature could serve as an independent prognostic factor; meanwhile, we draw the nomogram based on multivariate Cox regression (P<0.05). Compared to clinical variables, this signature's ROC curves demonstrated the second largest AUC value (0.737). The expression of these lncRNAs and the lncRNA signature are related to clinical stage, T stage, Lymph-node status, distant metastasis, KRAS mutation, BRAF mutation, MMR status, and perineural invasion. Finally, GSEA analysis results show that the signature is involved in six KEGG signal pathways, such as KEGG_HEDGEHOG_SIGNALING_PATHWAY, KEGG_ALPHA_LINOLENIC_ACID_METABOLISM, KEGG_ARACHIDONIC_ACID_METABOLISM, KEGG_CITRATE_CYCLE_TCA_CYCLE, KEGG_PENTOSE_PHOSPHATE_PATHWAY, KEGG_FRUCTOSE_AND_MANNOSE_METABOLISM. In conclusion, the current study shows a seven ferroptosis-related lncRNA signature could efficiently function as a novel and independent prognosis biomarker and therapeutic target for CRC patients. VL - 13 IS - 1 ER -
Respiratory Medicine, Huanggang Central Hospital Affiliated to Yangtze University, Huanggang, China
Department of Oncology, Huanggang Central Hospital Affiliated to Yangtze University, Huanggang, China
Department of Radiotherapy, Huanggang Central Hospital Affiliated to Yangtze University, Huanggang, China
Department of Oncology, Hunan Provincial People's Hospital, Changsha, China
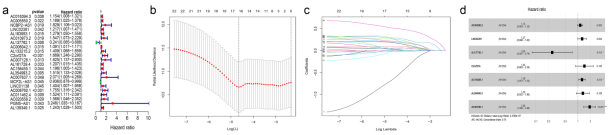
Figure 1. Construction of the ferroptosis-related lncRNAs prognostic signature. Univariate Cox regression (A), Lasso regression (B-C), Multivariate Cox regression (D).
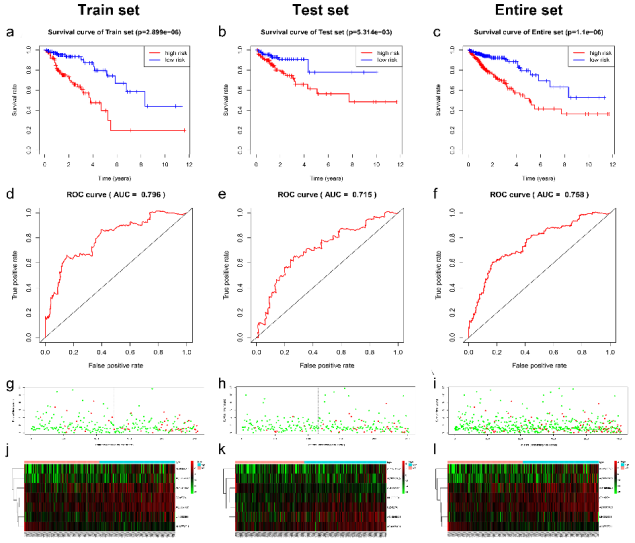
Figure 2. Validation and evaluation of the ferroptosis-related lncRNAs prognostic signature. Kaplan-Meier curves in the train set (A), test set (B), entire set (C); The AUC of three years dependent curve in the train set (D), test set (E), entire set (F); Survival status in high and low-risk patients for train set (G), test set (H), entire set (I), red dots represent death, and green dots represent alive; The cluster heat map of seven lncRNAs’ expression in high and low risk groups for the train set (J), test set (K), entire set (L).
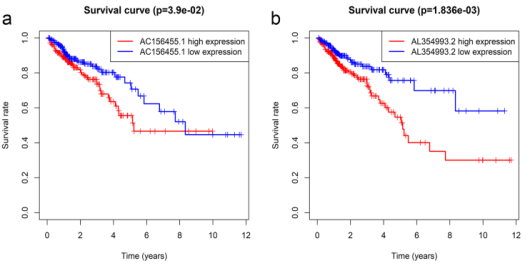
Figure 3. Two lncRNAs associated with overall survival in CRC patients using Kaplan–Meier curves and log-rank tests. The patients were stratified into high and low expression groups based on the median expression of each lncRNA. (A) AC026355.1. (B) AC099850.3.

Figure 4. The network relationship between the seven lncRNAs and ferroptosis genes. Prismatic represent lncRNA, and oval represent ferroptosis genes. The red line represents positive correlation, and blue represents negative correlation.
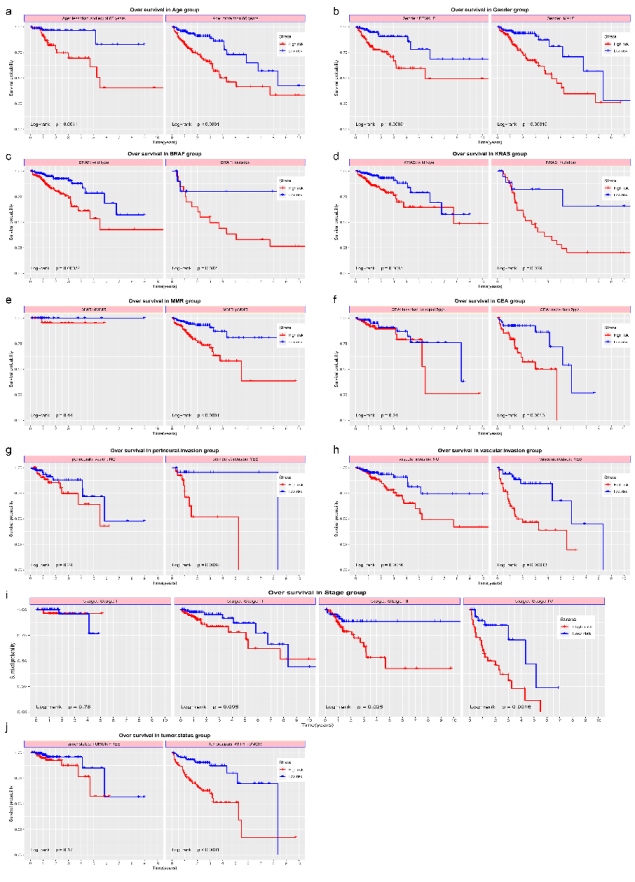
Figure 5. The overall survival of the ferroptosis-related lncRNAs prognostic signature in the stratification of clinical variables. Gender group (A), Age group (B), Stage group (C), KRAS group (D), BRAF group (E), MMR group (F), CEA group (G), Perineural invasion group (H), Vascular invasion group (I), Tumor status group (J).
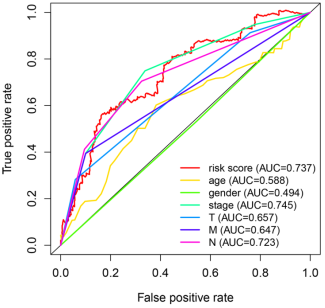
Figure 6. The ROC curve and nomogram of the ferroptosis-related lncRNAs prognostic signature. ROC curve compared to clinical variables (A), Nomogram (B).
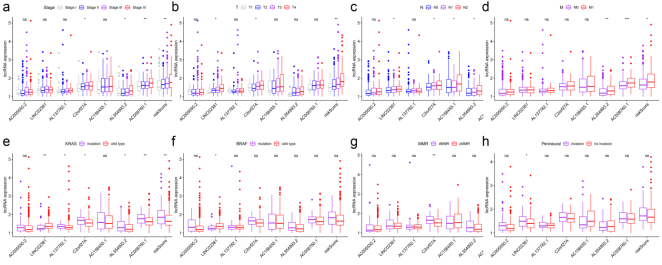
Figure 7. The correlation between the lncRNAs constituting the signature and clinical variables. Clinical stage (A), T stage (B), Lymph-node status (C), Distant metastasis (D), EGFR status (E), Eml4-Alk translocation status (F), KRAS status (G). * represents P<0.05, ** represents P<0.01, *** represents P<0.001, “ns” represents no statistical significance.
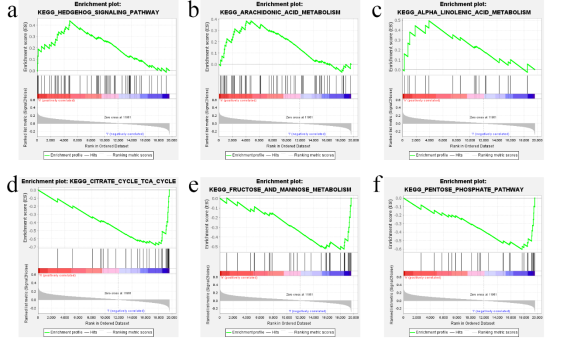
Figure 8. The KEGG enrichment analysis of GSEA enriched in the high-risk group and low-risk group of the ferroptosis-related lncRNAs prognostic signature. KEGG_HEDGEHOG_SIGNALING_PATHWAY(A), KEGG_ARACHIDONIC_ACID_METABOLISM(B), KEGG_ALPHA_LINOLENIC_ACID_METABOLISM (C), KEGG_CITRATE_CYCLE_TCA_CYCLE (D). KEGG_FRUCTOSE_AND_MANNOSE_METABOLISM(E), KEGG_PENTOSE_PHOSPHATE_PATHWAY(F)).

